
Research Open Access
Sherrie Xie, Jessica R. Meeker, Luzmercy Perez, Whitney Eriksen, Anna Localio, Hami Park, Alicia Jen, Madison Goldstein, Akua F. Temeng, Sarai M. Morales, Colin Christie, Rebecca E. Greenblatt, Frances K. Barg, Andrea J. Apter & Blanca E. Himes
Asthma Research and Practice volume 7, Article number: 13 (2021)
Abstract
Background
Exposure to fine particulate matter (PM2.5) increases the risk of asthma exacerbations, and thus, monitoring personal exposure to PM2.5 may aid in disease self-management. Low-cost, portable air pollution sensors offer a convenient way to measure personal pollution exposure directly and may improve personalized monitoring compared with traditional methods that rely on stationary monitoring stations. We aimed to understand whether adults with asthma would be willing to use personal sensors to monitor their exposure to air pollution and to assess the feasibility of using sensors to measure real-time PM2.5 exposure.
Methods
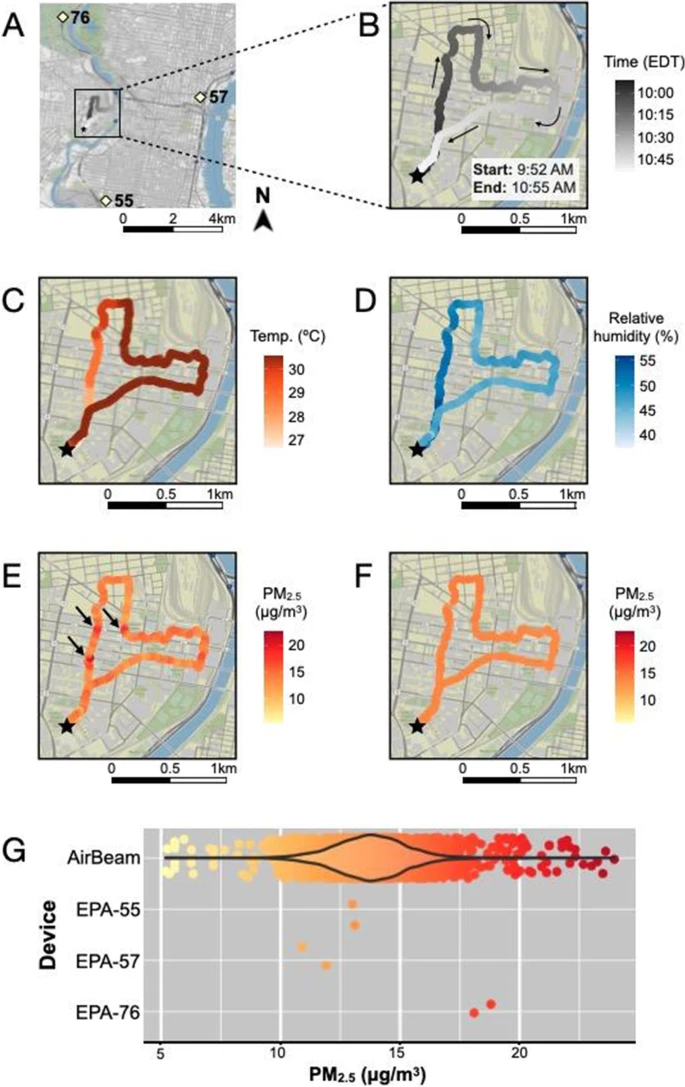
We conducted semi-structured interviews with 15 adults with asthma to understand their willingness to use a personal pollution sensor and their privacy preferences with regard to sensor data. Student research assistants used HabitatMap AirBeam devices to take PM2.5 measurements at 1-s intervals while walking in Philadelphia neighborhoods in May–August 2018. AirBeam PM2.5 measurements were compared to concurrent measurements taken by three nearby regulatory monitors.
Results
All interview participants stated that they would use a personal air pollution sensor, though the consensus was that devices should be small (watch- or palm-sized) and light. Patients were generally unconcerned about privacy or sharing their GPS location, with only two stating they would not share their GPS location under any circumstances. PM2.5 measurements were taken using AirBeam sensors on 34 walks that extended through five Philadelphia neighborhoods. The range of sensor PM2.5 measurements was 0.6–97.6 μg/mL (mean 6.8 μg/mL), compared to 0–22.6 μg/mL (mean 9.0 μg/mL) measured by nearby regulatory monitors. Compared to stationary measurements, which were only available as 1-h integrated averages at discrete monitoring sites, sensor measurements permitted characterization of fine-scale fluctuations in PM2.5 levels over time and space.
Conclusions
Patients were generally interested in using sensors to monitor their personal exposure to PM2.5 and willing to share personal sensor data with health care providers and researchers. Compared to traditional methods of personal exposure assessment, sensors captured personalized air quality information at higher spatiotemporal resolution. Improvements to currently available sensors, including more reliable Bluetooth connectivity, increased portability, and longer battery life would facilitate their use in a general patient population.