
Quint JK, Arnetorp S, Kocks JWH, Kupczyk M, Nuevo J, Plaza V, Cabrera C, Raherison-Semjen C, Walker B, Penz E, Gilbert I, Lugogo NL, van der Valk RJP; SABINA North American and European Study contributors. J Allergy Clin Immunol Pract. 2022 Mar 29:S2213-2198(22)00285-9. doi: 10.1016/j.jaip.2022.02.047.
ABSTRACT
Background
Expert national/global asthma management recommendations raise the issue whether a safe threshold of short-acting β2-agonist (SABA) use without concomitant inhaled corticosteroids (ICS) exists.
Objective
To examine SABA and maintenance therapy associations with severe asthma exacerbations across North America and Europe.
Methods
Observational analyses of 10 SABa use IN Asthma (SABINA) datasets involving 1,033,564 patients (≥12 years) from Canada, France, the Netherlands, Poland, Spain, United Kingdom (UK), and United States (US). Negative binomial models (incidence rate-ratio [95% confidence interval]) adjusted for prespecified-covariates]) evaluated associations between SABA and exacerbations.
Results
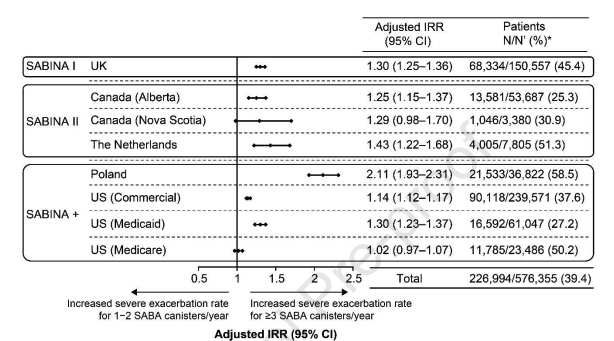
Across severities, 40.2% of patients were prescribed/possessed ≥3 SABA canisters/year. Per GINA-2018 definitions, step 3‒5-treated patients prescribed/possessing ≥3 vs. 1‒2 SABA experienced more severe exacerbations (between 1.08 [1.04‒1.13], US-Medicare; 2.11 [1.96‒2.27], Poland). This association was not observed in all step 1‒2-treated patients (the Netherlands 1.25 [0.91‒1.71]; US-commercial 0.92 [0.91‒0.93]; US-Medicare 0.74 [0.71‒0.76]). We hypothesize that this inverse association between SABA and severe exacerbations in the US datasets was attributable to the large patient population possessing <3 SABA and no maintenance therapy and receiving oral corticosteroid bursts without face-to-face healthcare provider encounters. In US SABA monotherapy-treated patients, ≥3 SABA was associated with more emergency/outpatient visits and hospitalizations (1.31 [1.29‒1.34]). Most GINA 2‒5-treated study patients (60.6%) did not have maintenance therapy for up to 50% of the time; however, the association of ≥3 SABA and severe exacerbations persisted (1.32 [1.18‒1.49]) after excluding these patients and the independent effect was further confirmed when UK SABA data was analyzed as a continuous variable in patients with up to 100% annual coverage for ICS-containing medications.
Conclusions
Increasing SABA exposure is associated with severe exacerbation risk, independent of maintenance therapy. As addressed by GINA, based on studies across asthma severities where as-needed fast-acting bronchodilators with concomitant ICS decrease severe exacerbations compared with SABA, our findings highlight the importance of avoiding a rescue/reliever paradigm utilizing SABA monotherapy.