
Francesco Menzella, Elena Bargagli, Maria Aliani, Pietro Bracciale, Luisa Brussino, Maria Filomena Caiaffa, Cristiano Caruso, Stefano Centanni, Maria D’Amato, Stefano Del Giacco, Fausto De Michele, Fabiano Di Marco, Elide Anna Pastorello, Girolamo Pelaia, Paola Rogliani, Micaela Romagnoli, Pietro Schino, Gianenrico Senna, Alessandra Vultaggio, Lucia Simoni, Alessandra Ori, Silvia Boarino, Gianfranco Vitiello, Elena Altieri & Giorgio Walter Canonica
Respiratory Research volume 23, Article number: 36 (2022)
Abstract
Background
Data from phase 3 trials have demonstrated the efficacy and safety of benralizumab in patients with severe eosinophilic asthma (SEA). We conducted a real-world study examining the baseline characteristics of a large SEA population treated with benralizumab in clinical practice and assessed therapy effectiveness.
Methods
ANANKE is an Italian multi-center, retrospective cohort study including consecutive SEA patients who had started benralizumab therapy ≥ 3 months before enrolment (between December 2019 and July 2020), in a real-world setting. Data collection covered (1) key patient features at baseline, including blood eosinophil count (BEC), number and severity of exacerbations and oral corticosteroid (OCS) use; (2) clinical outcomes during benralizumab therapy. We also conducted two post-hoc analyses in patients grouped by body mass index and allergic status. Analyses were descriptive only.
Results
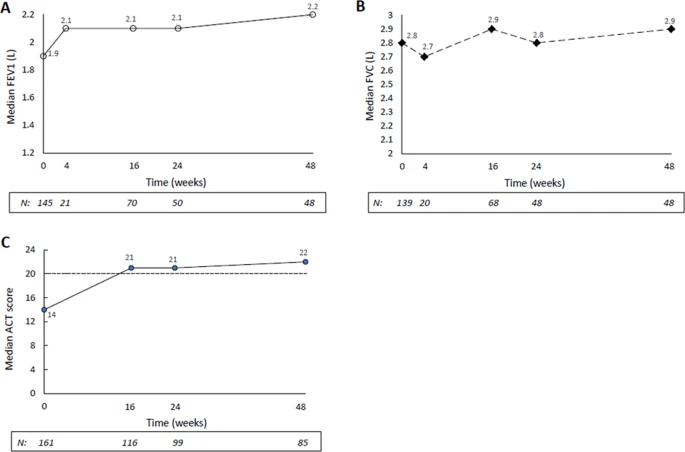
Of 218 patients with SEA enrolled in 21 Centers, 205 were evaluable (mean age, 55.8 ± 13.3 years, 61.5% females). At treatment start, the median BEC was 580 cells/mm3 (interquartile range [IQR]: 400–850); all patients were on high-dose inhaled controller therapy and 25.9% were on chronic OCS (median dose: 10 mg/die prednisone-equivalent [IQR: 5–25]); 92.9% experienced ≥ 1 exacerbation within the past 12 months (annualized exacerbation rate [AER] 4.03) and 40.3% reported ≥ 1 severe exacerbation (AER 1.10). During treatment (median duration: 9.8 months [IQR 6.1–13.9]; ≥ 12 months for 34.2% of patients), complete eosinophil depletion was observed; exacerbation-free patients increased to 81% and only 24.3% reported ≥ 1 severe event. AER decreased markedly to 0.27 for exacerbations of any severity (− 93.3%) and to 0.06 for severe exacerbations (− 94.5%). OCS therapy was interrupted in 43.2% of cases and the dose reduced by 56% (median: 4.4 mg/die prednisone-equivalent [IQR: 0.0–10.0]). Lung function and asthma control also improved. The effectiveness of benralizumab was independent of allergic status and body mass index.
Conclusions
We described the set of characteristics of a large cohort of patients with uncontrolled SEA receiving benralizumab in clinical practice, with a dramatic reduction in exacerbations and significant sparing of OCS. These findings support benralizumab as a key phenotype-specific therapeutic strategy that could help physicians in decision-making when prescribing biologics in patients with SEA.