
Colby Stong
About one-quarter of patients with mild asthma are not receiving therapy that is in line with recent guidelines published by the Global Initiative for Asthma (GINA) and the National Heart Lung and Blood Institute (NHLBI), according to study findings published in Allergy, Asthma & Clinical Immunology.
GINA and NHLBI guidelines were significantly updated in 2019 and 2020, respectively, to no longer recommend short-acting beta-agonists (SABA) as monotherapy for mild (GINA) or mild-persistent (NHLBI) asthma. Investigators sought to determine the extent to which these guidelines had been adopted in clinical practice through a retrospective chart review of electronic medical records of 30 hospitals and more than 300 clinics from a health system spanning 6 states in the western United States.
Charts were analyzed to assess how many patients with mild asthma were prescribed as-needed or daily inhaled corticosteroids (ICS) in addition to an as-needed SABA. Patients’ records were reviewed from July 1, 2021, to July 1, 2022. Participants were included if they were in primary care, aged 12 years or older, and had diagnosis codes indicating mild or mild persistent asthma.
The cohort included 1107 patients; of those, 284 patients (26%) did not have documentation of guideline-directed therapy for mild asthma and 823 (74%) were receiving guideline-directed therapy (difference, 48.7%; 95% CI, 45.1% to 52.3%; P <.001). Mean ages of patients were 42.4 years for nonguideline-adherent participants and 43.7 years for guideline-adherent participants (P =.353). Of the nonguideline-adherent participants, 61% were female compared with 62% of guideline-adherent patients.
Exacerbations occurred in 161 of the 1107 patients. Among the participants not receiving guideline-directed therapy, 12% had an exacerbation. For patients on guideline-directed therapy, 15.4% had an exacerbation. The difference in incidence of exacerbation between the 2 groups was not statistically significant (difference, –3.4%; 95% CI, –8% to 1.1%; P =.133).
Multivariate logistical regression analysis showed that asthma exacerbations decreased incrementally by 1.2% for each additional year of age (P =.006). Male patients were about 39% less likely to have an exacerbation compared with female patients (P =.01), and patients with gastroesophageal reflux disease were 63% more likely to have an asthma exacerbation (P =.02). Obese patients had a 73% higher likelihood of having an asthma exacerbation (P =.01), and patients with bronchitis were about 81% more likely to have an asthma exacerbation, although this was not statistically different (P =.082).
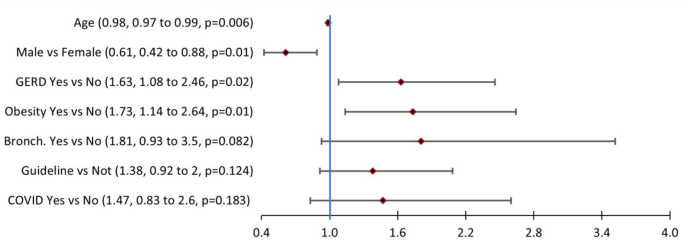
Factors associated with at least one asthma exacerbation
Patients with documented guideline-directed therapy were 38% more likely to have an asthma exacerbation, those with documented COVID-19 were 47% more likely, and those with bronchitis were 81% more likely (P =.124, P =.183, and P =.082, respectively).
Limitations include the sample size and the inability to correlate the timing of patient exacerbations and medication use. Also, it was difficult to determine which provider or facility was managing therapy because patients may have been visiting multiple facilities within the institution or outside the institution, and the number of asthma exacerbations for each patient was unknown.
“More work needs to be done to increase provider awareness regarding asthma guideline updates in outpatient and inpatient settings,” stated the study authors. They also said that “further studies in patients with mild asthma are needed to examine medication adherence, patient satisfaction, and exacerbation rate comparing patients on guideline-directed therapy versus those who are not.
References:

Zerr BA, Kruse JM, Glover JJ. Evaluation of adherence to guideline-directed therapy and risk factors for exacerbation in mild asthma: a retrospective chart review. Allergy Asthma Clin Immunol. 2024;20(1):27. doi:10.1186/s13223-024-00888-6